When I'm marking exams I see so many easy marks thrown away by students because of sloppy answering techniques so I thought I'd give an example of how I would answer a question - I'm not saying this is how
you should do it but just how
I do it.
This sort of question usually comes with questions like
- What is the blood group of this patient?
- Comment on the results
- What additional tests would you perform?
- What blood would you provide for this patient?
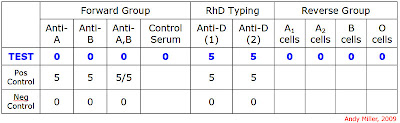
Before we begin - are all the controls present which should be and have they worked? All the controls are present and they have worked as expected so we have a valid test result - we can continue.
What is the blood group of this patient?
There is something wrong with these results so is there anything we can actually say? yes. We can say that this patient is RhD positive. We can't say that they are a group O because the reverse group does not agree with the forward group. We could hedge our bets and say that this patient "could be a group O" or "phenotypes as a group O in the forward / cell grouping" because this alerts the examiner that there is some doubt in your head about this group (which is a good thing).
Comment on the results
Here we are looking to see if you know what is wrong with the results and if you can give any sort of reasoned explanation as to why the results are the way they are.
In this case we can say that the patient's forward group tells us that they are a group O but if this was the case then we would expect to see anti-A and anti-B present in the patient plasma (reverse group) - we are not seeing this. This way you've alerted the examiner that you know what is wrong with these results and why they appear wrong to you - you have demonstrated your knowledge rather than relying on the examiners' telepathic powers - do not assume that an examiner can read your mind!
Now that you have pointed out what is wrong with the results are there any explanations as to why they are wrong? In this case there could be the following explanations:
- This patient could be a group O neonate who is yet to develop anti-A and anti-B in their reverse group
- This patient could be a very elderly person whose levels of plasma anti-A and anti-B have fallen to such an extent that they are now undetectable
- The patient could have agammaglobulinaemia or severely immunosuppressed and so be unable to make immunoglobulins (including anti-A and anti-B)
- The tester could have forgotten to put the patient plasma into the test
What additional tests would you perform?
This answer is governed by you explanations to the previous part of the question - this way you demostrate your reasoning behin your choice of tests rather than you are throwing the kitchen sink at the test in a hope that something may work!
You could suggest:
- Repeat the test to see if it was operator error
- Double the amount of patient plasma you use in the reverse group to see if you can detect very low levels of antibody in the patient
- Repeat the reverse group at 4C as ABo antibodies are IgM in natute and work better at lower temperature (displaying your knowledge again) - this should pick up low levels of antibodies
- Look at the patient's notes to see if they are a neonate or very old or suffering from some condition which could affect the test in a way demostrated by the results
Again, each response gives the examiner confidence that you know what you are talking about and that you are doing things for a reason.
What blood would you provide for this patient?
Here comes the difficult one - are you going to put the patient's safety at the top of your list or are you going to play chance with their life? Better to be safe than sorry and link it with your comments. Also, don't forget any other requisites for the blood if you talking about certain patient groups:
the phrase "I would not transfuse this patient until I was confident of their actual group" is always a winner but you could add, "In case of an emergency I would select group..."
Neonate: Group O RhD positive (include CMV-, HTO- / lysin - , irradiated)
Elderly: Group O RhD positive blood
Agammaglobulinaemia / immunosuppressed: Group O RhD positive irradiated blood (+CMV- perhaps)
As you can see I've done my best to explain why I've done what I've done - I have displayed my knowledge of a much wider subject area than just the ABO group to the examiner and not made them have to assume the reason why I've made the choices I have made - you don't get any marks for that! It is like the old comment in maths exams about "show your workings". This way, even if you get the answer wrong, the examiner can award you marks for the "way you were thinking" if it was in the right direction - just an answer which is wrong will give you no marks!
This explanation is a lot more long-winded than the actual process!
Try answering some questions for yourself and then looking at you answer and seing if it is obvious:
- why you have made the decisions you have made
- that you have demonstrated your knowledge
- that the examiner is in no doubt why you have done what you've done

 I cannot stress how much all of us involved in education, either on the teaching or on the learning side of things, should have some knowledge of Bloom's Taxonomy of Learning.
I cannot stress how much all of us involved in education, either on the teaching or on the learning side of things, should have some knowledge of Bloom's Taxonomy of Learning.



